The Hole Lies, the Rim Tells the Truth: What a Photograph of a Shattered Skull Really Reveals

How a cone in the bone gives away the direction of fire, an overlooked bone plug betrays the weapon class, and a bullet lighter than a coin destroys more than any fist
Photographs of skulls arrive on my screen, each with a single red circle around the spot the sender considers significant. Almost always, the circle is in the wrong place.
These images arrive regularly, each with a question attached. Is this a gunshot wound? Was it an arrow? Was this person beaten to death? Sometimes there is a ruler beside the bone, sometimes nothing at all beyond a guess. The pictures come from all over the world, from people with very different backgrounds, and they share one thing. The guess that comes with them is usually wrong, and it is wrong in a way that could be corrected in seconds if one only knew where to look.
I have worked with human remains ( The Skeleton Does Not Lie) for most of my life. I have held skulls with gunshot trauma in my hands, I have examined skulls where the final conclusion was that no shot had been fired at all, and I have learned that the one question almost everyone asks first is the least important of them all.
That question is: how big is the hole?
Forget the hole. The hole lies. The truth is written in the bone beside it. I will repeat that several times in this piece, across different calibers, across different wound patterns, because it is the single thought that carries everything else. Once you have internalized it, you will never look at a shattered skull the same way again.
The mistake almost everyone makes

Picture a windowpane with a stone flying through it. On the side the stone came from, the hole is small and relatively clean. On the other side the glass is blown out over a larger area, the fragments lie in the direction of flight, and the defect opens outward like a cone. Anyone who never saw the pane and only knows the two holes could never deduce from size alone which side the stone came from. Anyone who reads the fracture edges knows it instantly.
The human skull is that windowpane, except it has three layers. The outer surface is the outer table, the tabula externa, a compact plate of bone. The inner surface is the inner table, the tabula interna, also compact. Between them lies the diploë, a spongy layer riddled with cavities. When a bullet punches through this three-layered wall, it does not leave a symmetrical hole. It leaves a cone. And the direction in which that cone opens is the actual information.
At the entrance, the bullet blows away more bone on the inner surface than on the outer one. The defect is relatively small and sharply rimmed on the outside, and it widens into a cone on the inside. This phenomenon is called internal beveling. It is the most reliable anthropological sign of an entrance wound in cranial bone. Quatrehomme and Işcan studied this systematically in 1998 across a series of gunshot defects and found exactly this inner cone in 36 of 39 bones. In the overwhelming majority of cases, then, the bone tells you clearly where the bullet entered, provided you look at the inner surface rather than the outer one.
At the exit, everything reverses. Now the inner surface is the one struck first and left relatively intact, and the outer surface is blown outward. The cone opens to the outside, external beveling. The exit is typically larger than the entrance, more irregular in shape, with ragged edges. That is the rule, not a law of nature. The same study compared entrance and exit of the same shot and found the exit larger in most cases, with documented exceptions. After passing through, the bullet is deformed, unstable, tumbling, and it sheds its energy over a wider area.
Here lies the error in reasoning I encounter a thousand times. People measure the diameter of the dark opening and believe they can read the caliber from it. But at the exit, the dark opening is not the measure of the bullet, it is the measure of the destruction. And even at the entrance, the correlation between defect size and caliber is so weak that forensic science discarded caliber estimation from bone defects decades ago (DiMaio, 2016). In narrowly defined situations defect size can offer hints, but it is not a reliable measure of caliber. Too many variables interfere: skull thickness at the point of impact, angle of incidence, velocity, bullet construction, bone moisture. Measure the defect with a ruler, name a caliber, and you are not doing forensics. You are guessing, and guessing with a precision you do not have.
Here a distinction matters that constantly gets lost in lay reports, the one between a penetrating and a perforating wound. In this narrower sense, a penetrating cranial gunshot wound has an entrance but no exit, because the projectile remains in the body. A perforating wound has both an entrance and an exit. This distinction is not academic. If a skull carries only a single opening with internal beveling and no bullet remains inside, then the projectile must either have lodged in the long-decomposed soft tissue, or a perforating shot occurred whose second opening I have not yet found. The question of whether a skull bears one defect or two, and which is entrance and which is exit, decides the entire reconstruction of the bullet path. And it is the bullet path that ultimately speaks to life and death, not the diameter of any opening.
The fractures that weave the spider web
A bullet does not merely punch through bone; with sufficient energy, it can make the entire cranial vault burst. With sufficient energy, two kinds of fracture lines form, and their interplay is decisive for reconstruction.
The radiating fractures run outward from the defect like the spokes of a wheel, driven by the internal overpressure the bullet creates (Berryman & Symes, 1998). The concentric fractures, also called heaving fractures, run across them and connect the spokes into rings. Together they produce the spider web pattern everyone thinks they know from films, and which in reality rarely looks as tidy as it does on screen.
These lines are not mere decoration. They carry information that has been used in forensic medicine for over a century. A fracture line travels until it meets a pre-existing fracture, and there it stops. This is Puppe’s rule, named after Georg Puppe, who formulated the principle in 1903 (Geserick, Krocker & Wirth, 2012). For sequencing multiple cranial shots it remains in use (Madea & Staak, 1988). A remarkable consequence follows: with multiple shots, the sequence of impacts can often be reconstructed. The fracture lines of a later shot terminate when they encounter pre-existing fractures created by an earlier one. The younger line ends at the older, not the reverse. Which lines run uninterrupted and which are stopped reveals the chronological order. The bone keeps a record. You only have to be able to read it.
There is, however, a limitation I take seriously from my own casework. Fracture lines can also run through fresh surgical drill holes, for instance after an emergency craniotomy, and then the schematic application of the rule leads astray (Amadasi et al., 2022). Before sequencing multiple cranial injuries, the examiner must distinguish ballistic trauma from surgical intervention. That sounds obvious, but in practice the distinction is often missed.
That leaves the question of why a single fracture line changes direction several times before it runs out. It looks random. It is not. Bone breaks along its weak points, and the technical term for these weak points is stress risers (Love & Wiersema, 2016). A running fracture follows the path of least resistance, and that path is laid down by the anatomy of the individual skull (Berryman & Symes, 1998).
Four classes of structure shape the course. The first are the cranial sutures. For a long time the idea held that sutures reliably stop fractures. That is a simplification the evidence does not support. Fracture lines frequently cross sutures, sometimes run along them, and only sometimes end at them (Kriss, Morris & Martich, 2021). A suture is a zone of altered propagation, not a reliable barrier.
The second class are the foramina, the natural openings for vessels and nerves. Every opening weakens the bone locally and draws a running fracture toward it or deflects it.
The third class are the vascular grooves on the inner surface of the vault, above all the groove of the middle meningeal artery. This groove thins the bone, and a fracture follows it preferentially. If the artery tears in the process, the classic epidural hematoma forms, which is why fractures in the temporal region are so feared neurosurgically.
The fourth class is the thickness of the bone itself, which varies strongly across the vault. The temporal squama is the thinnest region of the neurocranium, on average around 2 millimeters, with documented individual values down to 1.2 millimeters (Rowbotham et al., 2023; Olatunji et al., 2018). The frontal and occipital bone are several times thicker. A fracture advancing into thin bone runs faster and farther. Meeting thick bone, it slows or deflects.
The pattern that emerges looks chaotic and is not. It is the mechanical signature of one individual skull, written in milliseconds. No two skulls are identical, and so no fracture pattern is like another, not even with the same weapon, the same distance, and the same point of impact. That is exactly what makes these lines so demanding to read, and their research value so large.
The exceptions that humble you
Anyone who works with skulls long enough learns respect for the cases that refuse to obey the textbook rule. It is precisely these exceptions that separate the expert from the hobbyist, because the hobbyist knows the rule and applies it rigidly, while the expert knows when it fails.
The keyhole defect is the most elegant of these exceptions. When a bullet strikes flat, that is tangentially, against the skull, it produces a defect that carries entrance and exit features in a single hole. The round part shows internal beveling, the attached wedge-shaped part shows external beveling. The whole thing looks like a keyhole, hence the name. For a long time the keyhole defect was regarded as a certain sign of a tangential shot. In the meantime, experimental work with micro computed tomography has shown that such defects can also arise from a perpendicular shot, through secondary and tertiary fractures (Dixon, 1982; Delannoy et al., 2016). The old certainty has fallen. The defect remains a strong indication of shot direction, but it is no longer proof, and anyone who still sells it as proof has not kept up with the research.
Even more treacherous is the rare case in which an entrance wound shows external beveling, that is, precisely the sign that normally marks the exit. Peterson documented a young man in 1991 with a perforating head wound from a high-velocity rifle in caliber 5.56 mm, whose entrance showed symmetrical external beveling. Reading cone direction rigidly here swaps entrance and exit and turns the entire reconstruction by 180 degrees. This is not a theoretical problem. In an expert opinion, this confusion can decide whether a shooter stood in front of or behind the victim.
And then there is taphonomy, the silent forger. Soil pressure, animal gnawing, root growth, recovery damage, all of this can leave defects on bone that resemble a gunshot. The literature describes a case in which a defect carried both internal and external beveling and yet came from no bullet at all, but from a sickle the perpetrator had used to move the body. Anyone who, on social media, blindly declares every round hole an entrance wound has never heard of this complexity. That is the real irritant in the whole business. Not that laypeople make mistakes, which is human. But that false findings are spread with a confidence that stands in inverse proportion to the knowledge behind them.
The bone plug, the evidence investigators overlook
There is a piece of evidence most investigators do not even know exists, and that is why it so often disappears into the grass, the leaves, or the soil. Forensics calls it the bone plug (Bird & Fleischman, 2015). It forms in the final instant of perforation, at the exit, and it carries information no other part of the finding provides.
When the bullet breaks through the bone from inside to outside, it punches a cone-shaped plug out of the vault and sheds fine fragments in the same moment. This dual mechanism is called plug and spall (Bird & Fleischman, 2015). The plug is not a random fragment, but a precise counterpart to the exit defect it came from. At the entrance the mirror image occurs: there the cone opens inward, and bone is driven into the cranial cavity rather than out of it. The intact recovered plug therefore typically comes from the exit.
Its shape follows the external beveling. On the inner side, the inner table, it is narrow. On the outer side, the outer table, it is wider, because the exit blasts the bone outward. The fracture edges distribute accordingly: the ectocranial surface carries tensile fractures, the endocranial surface stays smooth and intact (Bird & Fleischman, 2015). Hold such a plug to the exit and it fits almost perfectly.
This fit is forensically valuable. The wide side of the cone marks the exit direction and thus the direction of fire. More than that, a fully preserved plug reveals something about velocity. If the cone of bone stays intact instead of disintegrating into dust, the bullet lost much of its energy on the way through the skull and met the exit at low velocity (Bird & Fleischman, 2015). That is an indication of a slow weapon class, typically a small-caliber handgun, not a hard classification. What the plug does not reveal, by contrast, is the precise trajectory or the exact caliber, because the direction of most pronounced beveling is no reliable measure of either (Quatrehomme & Işcan, 1998).
The real problem is recovery. The plug separates from the skull during perforation and may lie some distance from the body, hidden by grass, leaves, or furniture. Viewed in isolation it looks like any bone fragment without context. If you do not know it exists, you do not pick it up. Well trained investigators search the suspected exit region and its surroundings, above all along the probable direction of fire, but also accounting for clothing, body position, and secondary displacement. In excavation settings this small fragment may be the only thing that documents the exit velocity and thereby the weapon class (Bird & Fleischman, 2015).
That this knowledge is no academic indulgence is shown by two finds from different continents. In the mass graves of Tuskulenai near Vilnius, holding victims of Soviet executions, an intact bone plug was found that could be assigned to a frontal exit and, through its low exit velocity, pointed to a small-caliber pistol (Bird & Fleischman, 2015). At the archaeological site of Puruchuco-Huaquerones in Peru a comparable fragment was documented, centuries old but readable by the same mechanics (M. S. Murphy et al., 2010).
The defect in the skull says that something passed through. The plug says in which direction and with what residual energy. Only the two together yield a complete picture, and that is why the small, easily overlooked piece of bone is often the most honest witness at the scene.
How close did the shooter stand?
From bone alone the shooting distance can hardly be determined, but from soft tissue and skin it can be determined very precisely, and because I am often sent photographs with tissue still attached, the short detour is worthwhile. Forensic medicine distinguishes four rough distance classes, and each leaves its own picture.
The contact shot, where the muzzle rests against the skin, is the most dramatic case. Here not only the bullet but the expanding propellant gases are driven into the body as well. If the muzzle sits over skin close to bone, as on the head, this gas drives between bone and skin, balloons the scalp from within and tears it open in a star shape. This star-shaped bursting, called stellate tearing, is a classic sign of a contact shot to the skull. Frequently the muzzle itself leaves an imprint on the skin, the so called muzzle imprint, because the gas-inflated skin is pressed back against the hot barrel mouth. Find a muzzle imprint and the matter is settled. Closer than contact is impossible.
The close-range shot leaves no muzzle imprint, but a halo of soot and unburned powder particles around the entrance. The soot sits only superficially and can be wiped away. The embedded powder grains cannot, they stick in the skin and create the characteristic tattooing, the stippling or powder tattooing (DiMaio, 2016). From the diameter of this halo and the density of the embedded grains the distance can be estimated, provided one knows or reconstructs the ammunition used. The boundaries between these distance classes are not fixed centimeter values: soot, powder tattooing, and muzzle imprint depend heavily on weapon, barrel length, ammunition, and load, and can differ considerably between weapon and ammunition combinations.
At contact and very near range there is one further phenomenon that plays a large role in crime scene work, back spatter. When the bullet enters and the temporary cavity tears the wound open from within, blood and the finest tissue are flung back against the direction of fire, that is, back toward the weapon and the hand that holds it. This back spatter can travel deep into the barrel and land on the shooter’s firing hand. In reconstructing an event this is worth its weight in gold, because the distribution of these fine droplets can, together with firing-hand residue, weapon position, bloodstain pattern, autopsy findings, and scene context, help to distinguish self infliction from homicide. The body leaves its own record, in an ink that is hard to forge.
The intermediate-range shot shows only the powder tattooing without dense soot, the distant shot finally only the pure mechanical defect with its typical abrasion collar. This abrasion collar is a narrow, abraded ring around the entrance that forms because the rotating bullet stretches and scrapes the skin edges as it enters. It is found at the entrance, not the exit, and is therefore a further distinguishing feature, though one that depends only loosely on bullet diameter. The collar says more about the geometry of impact than about caliber. Again the old lesson: the size of the opening is the least reliable quantity in the whole finding.
For forensic practice this distance determination is often more important than the caliber. A contact shot to the temple or the mouth speaks for a suicide or a killing at immediate range, a shot from several meters excludes self infliction in almost all cases, because the human arm simply has its reach. Here it is not the size of the hole that decides, but what lies on the skin around the hole.
The physics, without the lecture
To understand why different calibers leave such different pictures, one must grasp a single quantity. The kinetic energy of a bullet equals half the mass times the square of the velocity. The square is the decisive point. Velocity counts twice over, mass only once. Double the velocity and the energy quadruples. This is why a light, fast rifle bullet is more devastating than a heavy, slow pistol bullet, even though it weighs less.
In tissue this energy acts in two ways. The permanent cavity is the actual wound channel, the destroyed, crushed tissue along the path. The temporary cavity is a short lived radial stretching of the surrounding tissue that exists for only milliseconds and then collapses again. In elastic tissue like muscle this stretching largely springs back. In a rigid container, by contrast, the tissue can yield only to a limited extent to this rapid volume displacement (Fackler, 1996). And the most rigid container in the human body is the skull.
Here lies the key to the particular brutality of head shots with high-velocity ammunition. In the chest, tissue can yield. In the skull it cannot. The temporary cavity presses the brain against the inner wall of the bone, the pressure rises abruptly, and the cranial vault bursts from within. There is a rough rule of thumb for the velocity at which this effect becomes wounding, roughly 600 meters per second, often given in the anglophone world as 2000 feet per second. It is a rule of thumb, not a sharp boundary, and serious wound ballisticians stress that there is nothing magical about this number (MacPherson, 1994). But it roughly marks the threshold at which the bullet stops merely punching a hole and starts dragging the surrounding tissue along with it.
One more term that becomes important. A pointed bullet flies point first through the air and is stable. In denser tissue it loses this stability, begins to yaw, turns sideways and may tumble or break apart. It is precisely this yaw that decides how much energy is shed where, and it is the reason the same bullet can leave completely different wounds in two hits.
What bullet construction changes
Caliber alone says little. What matters far more is bullet construction, and this is where the categories diverge sharply.
The full-metal-jacket bullet carries a hard jacket around its lead core. It barely deforms, usually passes through its target completely and sheds part of its energy unused into the surroundings behind the target. Among its parties in international armed conflict, the Hague Declaration of 1899 prohibits bullets that easily expand or flatten in the body. Military ball ammunition has therefore traditionally used non-expanding full-metal-jacket designs, though reliability, penetration, and logistics also play their part. This has a macabre background. A full-metal-jacket bullet that passes through often causes more controlled wounds than an expanding one, which was considered more humane.
The soft point bullet and the hollow point bullet are the opposite. They are constructed to mushroom on impact, to enlarge their diameter substantially and their cross-sectional area, depending on construction, by a multiple, and thereby to shed far more energy in the target (DiMaio, 2016). The permanent cavity grows larger, the risk of through passage smaller. In modern civilian defensive ammunition, especially in the United States, expanding bullets are the norm.
Frangible ammunition is built to disintegrate on impact. Penetration depth and wound profile depend strongly on bullet construction, velocity, and target medium. At the trunk and extremities it often leaves large but shallow wounds, because the fragments in soft tissue frequently do not penetrate deeply enough to reach central structures. In the skull this rule of thumb does not hold without qualification: the closed bony system can redirect fragment energy internally and produce widespread intracranial damage that far exceeds what the external wound picture suggests.
And then there is wadcutter ammunition, the favorite of target shooters. It is a cylindrical lead bullet with a flat nose and a sharp shoulder edge. This edge punches a clean, circular hole in the paper target instead of stretching and tearing it like a round-nose bullet, which makes scoring easier. Forensically this is highly relevant, because the same sharp edge punches a characteristically clean hole in skin too. An experimental study at the University of Freiburg measured this. The entrance diameter of a wadcutter averaged 8.43 millimeters, that of a round-nose bullet of the same caliber only 4.43 millimeters (Pircher et al., 2017). For bone a comparable effect is plausible, but it must be assessed separately from the osseous beveling and the local bone structure. The wadcutter, then, makes the largest hole with the smallest abrasion. Judge by hole size alone, not knowing this, and you overestimate the caliber massively. The hole again. The wrong spot again.
The gallery of calibers
Now to the actual cartridges, and I begin with the handguns, because they are the most common.
The 9 millimeter, more precisely 9 × 19 mm Parabellum, is the most widespread pistol caliber in the world. Georg Luger developed it at the start of the 20th century, and the German army adopted it in 1908 with the Pistole 08. The bullet diameter is around 9 millimeters, the muzzle velocity 340 to 400 meters per second, that is, near subsonic to slightly supersonic. As a full metal jacket it usually passes through, as a modern hollow point it sheds its energy in a controlled way. It is the workhorse, not the specialist. And it is, this belongs to the sad statistics of the topic, the caliber I encounter most often in forensic practice, simply because it is the most widespread.
The .45 ACP is the American answer to the same task, designed by John Browning around 1905. It has a bullet diameter of 11.4 millimeters, so it is considerably thicker, but slower, around 250 to 290 meters per second, clearly in the subsonic range. Heavy, slow bullet against a lighter, faster one. The dispute over which of the two is better is as old as the calibers themselves, and DiMaio, one of the authoritative forensic pathologists, observed dryly that there is no appreciable difference in the effectiveness of the two (DiMaio, 2016). What makes the .45 interesting for forensic assessment is its diameter. With a fully preserved, undeformed bony primary defect, a channel substantially narrower than the nominal diameter of the .45 ACP can serve as a cautious exclusion indicator. But this argument holds only under that limiting condition: a bullet that has been deflected, tumbling, or deformed before impact can produce defects smaller than its nominal diameter would suggest. Here, and only under this restriction, does hole size provide an argument, and even then only at the actual channel, not at the surrounding field of destruction.
The .22 Long Rifle, the classic small bore, is the great misunderstanding among calibers. It is tiny, the bullet diameter is about 5.6 millimeters, the energy is low, in some weapons only 65 to 190 joules. This very weakness makes it forensically peculiar. The bullet often does not have enough energy to leave the skull again. It stays inside. And worse, it can ricochet off the inside of the opposite skull wall and travel through the brain a second time, an intracranial ricochet. Kirkpatrick and DiMaio found in a series of fatal .22 cases that the bullet remained in the skull in 83 percent (Kirkpatrick & DiMaio, 1978). Here a lesson shows itself that this whole article carries. Small does not mean harmless, and large does not mean deadlier. The energy and its path through the tissue decide, not the diameter.
The small bore has a dark chapter I want to spend more time on than usual. American intelligence used the High Standard HDM during the early Cold War, a suppressed .22 pistol developed originally for the OSS. Israeli intelligence preferred the Beretta 71 in the same caliber. The forensic logic discussed for such weapons runs to low report, limited overpenetration, and lethality only at very close range.
Hollywood has distilled this combination into a myth that refuses to die. A suppressor does not make a weapon silent. It suppresses. A gunshot produces two sounds: the muzzle blast generated by expanding propellant gases leaving the barrel, and the sharp supersonic crack the bullet makes the instant it breaks the sound barrier at roughly 343 meters per second. The suppressor slows and cools the escaping gas through a system of chambers and baffles, reducing the muzzle blast, sometimes substantially. The supersonic crack of the bullet it cannot touch. A suppressed pistol sounds in a film like a dry sigh. In reality it sounds like a sharp handclap with a metallic edge, loud enough to make heads turn.
Standard .22 LR high-velocity cartridges leave the barrel at 365 to over 400 meters per second, squarely supersonic, and produce that crack in every case. Subsonic ammunition is engineered differently: reduced propellant charge, often a heavier bullet, muzzle velocity held reliably below 320 meters per second. No supersonic crack. The combination of suppressor and subsonic .22 brings total noise to roughly 110 to 120 decibels. That sounds modest until you know that a thunderclap or a starting chainsaw lands in the same range. In a very well-configured setup, the mechanical noise of the cycling bolt can make up a substantial part of the perceived total sound. Nothing like the soundless weapon no one in a thriller ever hears.
The Soviets arrived at the same destination by a different route. The KGB used the PB pistol, an integrally suppressed weapon chambered in 9 × 18 mm Makarov, with a muzzle velocity of around 290 meters per second, inherently subsonic without any special ammunition. Different caliber, same idea: no supersonic crack, suppressed muzzle blast, minimum audible signature.
The brainstem is the structure on which everything depends. Severe injury to it is generally incompatible with survival, because it disrupts the centers that control respiration and circulation. That is the cold physiology behind why such wounds are so rapidly fatal, and I describe these weapons only because they appear in the historical and forensic record.
It is to be kept sharply separate from the National Socialist neck shot installations in the concentration camps, institutionalized killing techniques using firearms, often disguised as a medical measurement. Weapons, calibers, and concrete execution varied by installation and period. Two different things, often confused, and I name them only to forestall the confusion.
Now to the rifles, and here the physics I spoke of above becomes visible.
The .308 Winchester and the militarily closely related 7.62 × 51 mm NATO are the heavy standard rifle caliber. Bullet diameter 7.62 millimeters, bullet mass usually 9.5 to 11.7 grams, muzzle velocity around 830 to 860 meters per second, muzzle energy about 3,500 joules. The Bundeswehr fields it in the designated marksman rifle G28, a precision weapon based on the Heckler and Koch HK417 for which the manufacturer quotes a group of roughly 45 millimeters at 100 meters as a factory guarantee under standardized test conditions, a figure that reflects laboratory testing rather than field performance. The marksmen of the GSG 9 also use the G28. In police service the Remington 700 in .308 is widespread. An interesting detail from wound ballistics: the 7.62 NATO bullet formerly manufactured in Germany, with a thinner steel jacket, fragmented considerably more than the American version with its thicker copper jacket. Half a millimeter of jacket thickness decides whether a bullet passes through or breaks apart in the target.
The .50 BMG, the 12.7 millimeter caliber, is in a class of its own for range and energy. Bullet mass around 42 grams, muzzle velocity around 850 meters per second, muzzle energy between 14,000 and 20,000 joules depending on the load, fielded for instance in the Barrett, designated M107 in the US Army. It is a caliber against materiel and across great distances. At this point I clear up a popular error that I encounter again and again. The 2,475-meter shot fired by a British soldier in Afghanistan in 2009, for years cited as one of the longest confirmed sniper kills, did not come from a .50 BMG. It came from a rifle in caliber .338 Lapua Magnum. This is constantly misattributed, and anyone who wants to get it right should get it right.
Such skulls are considered rare in civilian forensic practice. That is true for the day-to-day work of criminal investigation. Anyone who believes, however, that a human skull carrying a gunshot wound is an outright rarity is badly mistaken. Gunshot injuries are found not only at the skull but at every bone that happened to be in the way: ribs, scapula, pelvis, limbs. The Second World War cost between 21 and 25 million soldiers their lives. The Soviet Union alone lost roughly 8.7 to 10.7 million soldiers, Germany 5.3 million. Adding the 9 to 11 million military dead of the First World War brings the total to 30 to 36 million fallen soldiers in less than 30 years, a substantial proportion of them from firearms injuries. The remains exist in museums, university collections, with forensic anthropologists, and in private skull collections of a scale that would surprise most people. They also lie still in the ground. Along the former Eastern Front between Leningrad and Stalingrad, skeletons are still being washed out of the soil today by erosion and the spring thaw. More than 42,000 volunteers search across Russia for the remains of the war dead. The Ingria group alone, working around Sinyavino, has recovered over 3,000 soldiers in 20 years.
Anyone who comes across a photograph of a skull with a gunshot wound online should not panic. Most of these images show no current criminal case, but teaching material, collection specimens, or war casualties not yet given a proper burial. The reflex to immediately construct a homicide is understandable. Statistically speaking, it is usually wrong.
The small bullet that is deadlier than a fist


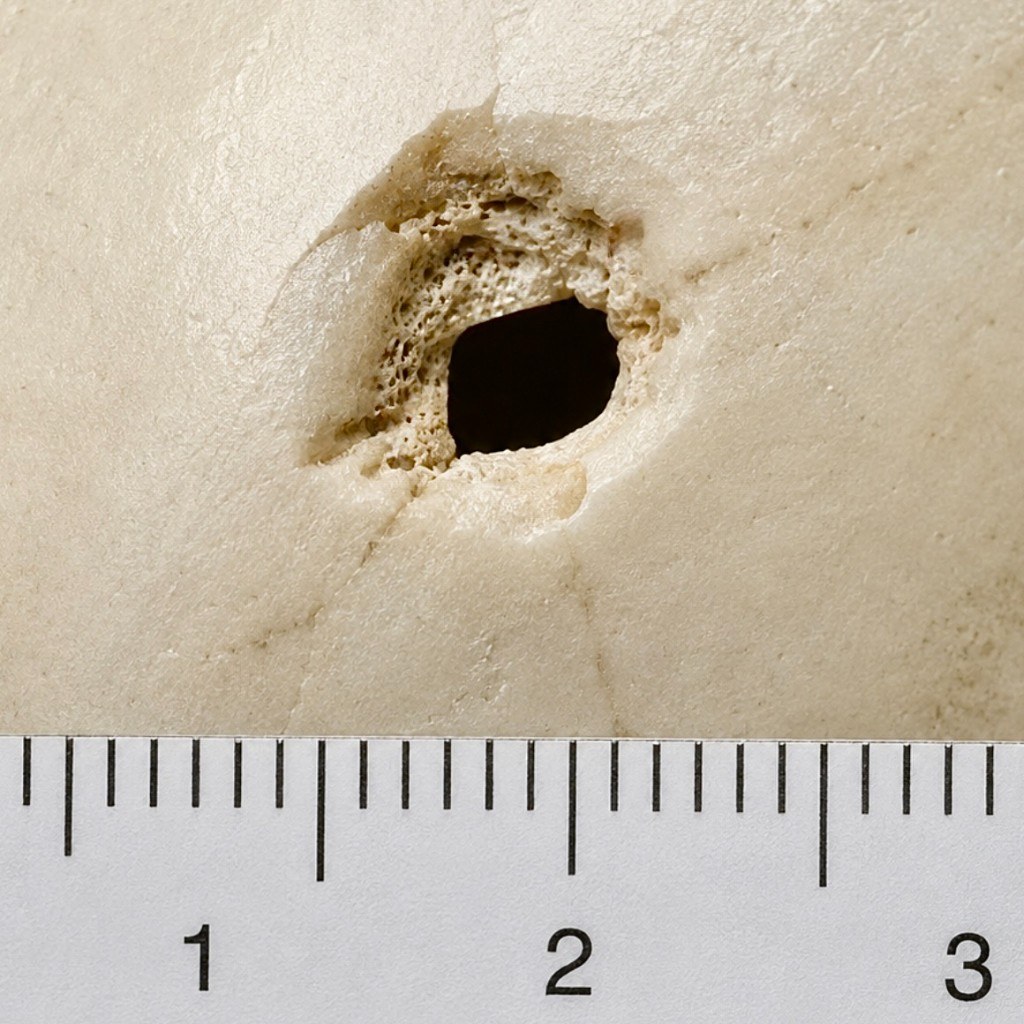
Two photographs accompany this article. The first shows a human skull with a defect pattern that fits well with an exit injury from a small, fast rifle bullet: external beveling at the os parietale, a fragmented outer table, radiating fracture lines that reach far beyond the actual defect. The perforation channel itself, the dark hole, is small, roughly 7 to 8 millimeters. The damage pattern around it is enormous. A caliber-certain attribution from the bone finding alone is not possible. The pattern would be compatible, for example, with high-velocity ammunition in the range of .223 Remington or 5.56 × 45 mm NATO, provided impact velocity, bullet construction, and fragmentation behavior were appropriate. The second photograph shows no confirmed incident projectile but a comparison projectile from this caliber range, a full metal jacket of .224 inch diameter, documented on a forensic ABFO scale. Small hole, enormous damage picture. This combination is the signature of a fast, unstable, fragmenting bullet.
The nominal caliber of the .223 is 5.56 millimeters, though the actual bullet diameter is .224 inch, about 5.7 millimeters. The bullet weighs between 3.6 and 4 grams, that is, less than a two-euro coin. But it leaves the barrel at over 900 meters per second. And in tissue it does something that the wound ballistician Martin Fackler described in meticulous detail in a famous paper from 1989 (Fackler, 1989). The bullet first flies about 12 centimeters point first, then it begins to yaw violently, turns sideways, and at the cannelure, the crimping groove, it breaks apart. The front part keeps about 60 percent of the mass, the rear disintegrates into a swarm of small fragments that scatter up to 7 centimeters radially. These fragments pre-weaken the tissue, and into this pre-weakened tissue the temporary cavity then presses. Fackler’s description applies primarily to the military M193 full metal jacket and comparable high-velocity loads at sufficient impact velocity. Civilian .223 loads, soft-point bullets, and lead-free hunting projectiles can produce markedly different wound profiles, as can hits beyond the fragmentation threshold, meaning at greater distance or from a shorter barrel. Both effects together produce a permanent cavity many times what the tiny bullet diameter would lead one to expect. This is the mechanism behind the large, seemingly disproportionate wounds observed in the Vietnam War with the first M16 rifles, which caused a stir at the time.
A careful look raises the question why exit wounds sometimes appear oval or elongated rather than round. The answer lies in yaw. If the projectile begins to tumble before it strikes the inner table from within, it does not punch through with its circular cross-section but obliquely. The result is an oval or elongated defect that mirrors the orientation of the bullet at the moment of impact. Depending on shot angle and distance, this yaw may be more or less pronounced. Quatrehomme and Işcan documented in their series that exit wounds can be round, oval, square, and rectangular (Quatrehomme & Işcan, 1998). That sounds like a diagnostic problem. It is not. The entrance usually stays circular, because the bullet is still stable and flying point-first at the entry point. The overall picture of a round entrance with internal beveling and an oval or irregular exit with external beveling is internally consistent and forensically readable regardless of the precise shape of the exit defect. Shot angle and distance change the geometry of the hole. They change nothing about the readability of the finding.
Myths surround this bullet, and one of them is genuinely contested, which is why I honestly mark it as contested. There is the thesis that a .223 hit could kill by a conducted pressure wave alone, a so called hydrostatic shock, even with a hit to a limb far from vital organs. On one side stand wound ballisticians like Fackler, who regard this as a myth and argue that there are only two wound mechanisms, crushing and stretching, and that everything else is folklore. Fackler liked to point to the kidney stone lithotripter, which produces stronger pressure waves than most bullets without damaging soft tissue. On the other side stand researchers like the Courtneys, who bring evidence of remote effects into the field, for instance a rise in blood pressure in the brain after a hit to the thigh, the evidential weight of which remains contested (Courtney & Courtney, 2008). A broad scientific consensus does not exist to this day. To claim that the lethality of the .223 rests securely on a shock wave goes beyond the evidence. What is undisputed, by contrast: in the enclosed space of the skull itself, the temporary cavity produces a devastating internal pressure and bursting fractures. In the skull, the .223 needs no contested remote-effect mechanism. Its near effect is entirely sufficient.
With this the circle closes back to the beginning. The caliber that left the smallest opening in the photograph is one of the most destructive of all. Measure only the hole and you would never arrive at it. Read the bone around it and you see it at once.
Why some survive
There is a notion that persists stubbornly, that a head shot is synonymous with certain death. That is not true. It is very often fatal, and the numbers are sobering. The neurosurgical literature offers no comfort for those expecting quick reassurance: between 66 and 90 percent of patients with penetrating head wounds do not survive transport to a hospital (Qi & Li, 2021). Among those who arrive alive, up to half survive in some series.
What it depends on has been worked out by a large meta analysis of 1,774 patients (Maragkos et al., 2018). Decisive are the neurological state on arrival, measured by the Glasgow Coma Scale, the reaction of the pupils, and above all the path of the bullet through the brain. Bilaterally fixed, dilated pupils unresponsive to light are an extremely unfavorable sign. A path that crosses both hemispheres of the brain is considerably more dangerous than one that stays within a single hemisphere. A path through the ventricles worsens the prognosis substantially. And a shot fired with suicidal intent has a statistically higher mortality, for sad reasons I will come to shortly.
How sharply these boundaries run is shown by an older but methodically sound series of 49 small-bore shots to the brain (Suddaby, Weir & Forsyth, 1987). Overall mortality was 61 percent. Among patients who arrived with largely preserved consciousness, that is, a high value on the Glasgow Coma Scale, none died. Among deeply unconscious patients with a value of seven or below, 85 percent died. And every patient with bilaterally fixed, dilated pupils died in this series without exception. A French series confirmed the same finding from the other side. Comatose patients without brainstem signs survived in over a third of cases, comatose patients with brainstem signs in not a single case of that cohort (Shoung, Sichez & Pertuiset, 1985). It comes down, as so often with head shots, to a single structure. If the brainstem is spared, there is a chance. If it is struck, there is none.
There are two constellations in which survival becomes considerably more likely. The first is the graze, the tangential gunshot wound. If the bullet grazes the skull without breaching the inner table of bone, the protective vault remains intact. Such injuries look dramatic but are often survivable. Harmless they are not. In a large series, 16 percent of these patients nonetheless had skull fractures and a quarter had intracranial bleeding, some deteriorating only hours later (Anglin et al., 1998). Anyone who survives a graze to the head belongs under observation, not discharge.
The second constellation is the shot through the mouth directed forward and upward.
The comrade in the ammunition depot
I am a veteran. I served four years with the German Air Force, including at Fighter-Bomber Wing 49 in Fürstenfeldbruck. In 1992 a comrade there tried to take his own life in an ammunition depot with his service weapon. The shot passed through the mouth, directed forward and upward.
On that day an American military helicopter was visiting the base. They flew into the depot, a wooded stretch of ground, and got him out with a daring landing among the trees, to fly him to a hospital. After that there was an absolute news blackout. We learned nothing. Only months later, I believe it was almost a year, the information reached me that he had survived. Blind in one eye, with a slight speech impairment, but he was alive.
I was there when we pulled him from the toilet. I had my hand on his head. And under my grip I felt the skull give way. I carry that feeling within me to this day, and in the decades since I have learned enough about anatomy to understand why this man survived and why it felt the way it felt.
A shot through the mouth directed forward and upward takes a path through the frontal lobe. The frontal lobe is, neurologically speaking, a comparatively silent region. That does not mean an injury there is harmless, but that the centers which directly govern breathing and circulation do not lie here. The bony barrier of the anterior cranial fossa partly shields the brainstem lying beneath and behind it from the downward-directed pressure. This is exactly why some people survive an intraoral shot, often with severe injuries to the eyes, the face, the speech, but they survive. A study of 157 cases found that mortality depends strongly on the entrance site: with shots to the temple 82 percent, with submental and intraoral shots by contrast only 30 percent (J. A. Murphy et al., 2016; Kriet, Stanley & Grady, 2005). The giving way under my hand was the fractured but not destroyed frontal region. Had the bullet taken another path, I would not be writing this article.
The cold anatomy and the warm human being coincide in such moments. This one man taught me more about the line between surviving and dying than many a lecture.
What remains
Gunshot wounds to the skull are, forensically considered, a readable text. The cone reveals the direction. The fractures reveal the sequence. The soot and the muzzle imprint reveal the distance. The path reveals the prognosis. And the hole, which almost everyone measures first, reveals the least of all. Learn to read the bone instead of the hole and you see in seconds what stays hidden from others, correcting in a single sentence what has been passed around wrong online for years. There is no magic in this, and no talent. It is method, practiced on enough cases until the eye wanders to the right spot of its own accord, away from the hole, toward the rim, toward the fracture edge, toward that narrow ring of abraded skin that tells more than the entire dark crater at its center.
In many forensic settings, and certainly in mine, most gunshot wounds to the human skull that reach casework are not homicides. They are suicides. In 2024, 10,372 people in Germany took their own lives, slightly more than the year before and noticeably more than the ten year average (Statistisches Bundesamt, 2025). The distribution has been alarmingly constant for years. Around 71 percent are men. Gender-specific suicide rates show that men are affected more than twice as often as women, with the gap considerably wider in certain age groups.
Behind this number stands a pattern the research knows well. Economic hardship, unemployment, financial pressure drive the suicide rate upward, and they hit men of working age particularly hard. A meta analysis showed a markedly elevated relative risk under unemployment, more pronounced in men than in women (Milner, Page & LaMontagne, 2014). And added to this is the silence. Men seek help less often, speak less often about strain, pause less often, because they have learned that strength means showing nothing. They carry it alone until they can carry it no longer.
I find that sad, and I say it as someone who works with the bony consequences of this silence. The skull that lies on my table in the end, or appears on a photograph in my inbox, almost always belonged to a person whom at some point no one listened to anymore, or who no longer asked anyone. Forensics can reconstruct what happened. It cannot prevent it from happening. Only people can do that, people who listen to one another before the bone gets the last word.
If you are reading this and in a dark place yourself, help is there around the clock, anonymous and free. In the United States, call or text 988, the Suicide and Crisis Lifeline, or 911 in immediate danger. In Germany, call 112 in an emergency, or the Telefonseelsorge at 0800 111 0 111, 0800 111 0 222, or 116 123. Elsewhere, the directory at findahelpline.com points to local crisis support. Talking is no sign of weakness. It does not solve everything at once, but it shifts the moment, creates connection, and can save lives.
References
- Quatrehomme, G., & Işcan, M. Y. (1998). Analysis of beveling in gunshot entrance wounds. Forensic Science International, 93(1-2), 45-60.
- Quatrehomme, G., & Işcan, M. Y. (1998). Gunshot wounds to the skull: Comparison of entries and exits. Forensic Science International, 94(1-2), 141-146.
- Berryman, H. E., & Symes, S. A. (1998). Recognizing gunshot and blunt cranial trauma through fracture interpretation. In K. J. Reichs (Ed.), Forensic Osteology: Advances in the Identification of Human Remains (2nd ed., pp. 333-352). Charles C Thomas.
- Dixon, D. S. (1982). Keyhole lesions in gunshot wounds of the skull and direction of fire. Journal of Forensic Sciences, 27(3), 555-566.
- Delannoy, Y., Colard, T., Le Garff, E., Humez, S., Gosset, D., & Hedouin, V. (2016). The mechanism of the keyhole lesion reassessed: An experimental approach. Journal of Forensic and Legal Medicine, 37, 1-7.
- Peterson, B. L. (1991). External beveling of cranial gunshot entrance wounds. Journal of Forensic Sciences, 36(5), 1592-1595.
- Anglin, D., Hutson, H. R., Luftman, J., Qualls, S., & Moradzadeh, D. (1998). Intracranial hemorrhage associated with tangential gunshot wounds to the head. Academic Emergency Medicine, 5(7), 672-678.
- DiMaio, V. J. M. (2016). Gunshot Wounds: Practical Aspects of Firearms, Ballistics, and Forensic Techniques (3rd ed.). CRC Press.
- Fackler, M. L. (1989). Wounding patterns of military rifle bullets. International Defense Review, 22(1), 59-64.
- Fackler, M. L. (1996). Gunshot wound review. Annals of Emergency Medicine, 28(2), 194-203.
- Courtney, M. W., & Courtney, A. C. (2008). Scientific evidence for hydrostatic shock. arXiv preprint arXiv:0803.3051.
- MacPherson, D. (1994). Bullet Penetration: Modeling the Dynamics and the Incapacitation Resulting From Wound Trauma. Ballistic Publications.
- Pircher, R., Geisenberger, D., Pollak, S., Perdekamp, M. G., & Thierauf-Emberger, A. (2017). The influence of the bullet shape on the width of abrasion collars and the size of gunshot entrance holes. International Journal of Legal Medicine, 131(2), 437-443.
- Maragkos, G. A., Papavassiliou, E., Stippler, M., & Filippidis, A. S. (2018). Civilian gunshot wounds to the head: Prognostic factors affecting mortality. Meta-analysis of 1774 patients. Journal of Neurotrauma, 35(22), 2605-2614.
- Qi, H., & Li, K. (2021). Civilian gunshot wounds to the head: A case report, clinical management, and literature review. Chinese Neurosurgical Journal, 7(1), 12.
- Suddaby, L., Weir, B., & Forsyth, C. (1987). The management of .22 caliber gunshot wounds of the brain: A review of 49 cases. Canadian Journal of Neurological Sciences, 14(3), 268-272.
- Kirkpatrick, J. B., & DiMaio, V. (1978). Civilian gunshot wounds of the brain. Journal of Neurosurgery, 49(2), 185-198.
- Shoung, H. M., Sichez, J. P., & Pertuiset, B. (1985). The early prognosis of craniocerebral gunshot wounds in civilian practice as an aid to the choice of treatment. A series of 56 cases studied by computerized tomography. Acta Neurochirurgica, 74(1-2), 27-30.
- Kriet, J. D., Stanley, R. B., & Grady, M. S. (2005). Self-inflicted submental and transoral gunshot wounds that produce nonfatal brain injuries: Management and prognosis. Journal of Neurosurgery, 102(6), 1029-1032.
- Murphy, J. A., Lee, M. T., Liu, X., & Warburton, G. (2016). Factors affecting survival following self-inflicted head and neck gunshot wounds: A single-centre retrospective review. International Journal of Oral and Maxillofacial Surgery, 45(4), 513-516.
- Milner, A., Page, A., & LaMontagne, A. D. (2014). Cause and effect in studies on unemployment, mental health and suicide: A meta-analytic and conceptual review. Psychological Medicine, 44(5), 909-917.
- Statistisches Bundesamt (Destatis). (2025). Todesursachenstatistik, reporting year 2024. Final results, published October 2025.
- Bird, C. E., & Fleischman, J. M. (2015). A rare case of an intact bone plug associated with a gunshot exit wound. Journal of Forensic Sciences, 60(4), 1074-1077.
- Murphy, M. S., Gaither, C., Goycochea, E., Verano, J. W., & Cock, G. (2010). Violence and weapon-related trauma at Puruchuco-Huaquerones, Peru. American Journal of Physical Anthropology, 142(4), 636-649.
- Love, J. C., & Wiersema, J. M. (2016). Skeletal trauma: An anthropological review. Academic Forensic Pathology, 6(3), 463-477.
- Kriss, S., Morris, J., & Martich, V. (2021). Pediatric skull fractures contacting sutures: Relevance in abusive head trauma. American Journal of Roentgenology, 217(1), 218-222.
- Rowbotham, S. K., Mole, C. G., Tieppo, D., Blaszkowska, M., Cordner, S. M., & Blau, S. (2023). Average thickness of the bones of the human neurocranium: Development of reference measurements to assist with blunt force trauma interpretations. International Journal of Legal Medicine, 137(1), 195-213.
- Olatunji, R. B., Efidi, R. C., Uko, E. E., & Ogunseyinde, A. O. (2018). Thickness and texture of the squamous temporal bone in a Nigerian tertiary hospital. West African Journal of Radiology, 25(2), 112-117.
- Madea, B., & Staak, M. (1988). Determination of the sequence of gunshot wounds of the skull. Journal of the Forensic Science Society, 28(5-6), 321-328.
- Geserick, G., Krocker, K., & Wirth, I. (2012). Puppe’s rule: A literature review. Archiv für Kriminologie, 229(1-2), 34-43.
- Amadasi, A., Franceschetti, L., Magli, F., Muccino, E. A., Mazzarelli, D., & Cattaneo, C. (2022). Two peculiar cases of cranial fractures running through craniotomy burr holes. International Journal of Legal Medicine, 136(4), 1177-1180.

The Skeleton Does Not Lie
What a skull on the piano gives away about a stranger's life, why bone is more honest than…

Otto Sapiens, the Last Model Before Extinction
A diagnosis of the Stone Age brain under the screen, the voluntary surrender of thought, and the single…
Probability Zero: Why Our Genome Could Not Have Arisen by Chance
A forensic expert presents the mathematical case against the chance origin of the human genome, working through protein…