Reading Age from the Skull: Cranial Sutures and What Forensic Anthropology Can Actually Deliver

How Cranial Sutures Became the Most Argued-Over Millimeter in Forensic Anthropology, Why a Century of Practitioners Could Not Agree on Their Reliability, and What That Tells Us About the Gap Between What Courts Want and What Bones Can Actually Deliver
The medical examiner looked at me the way medical examiners look at forensic consultants who have just delivered something less crisp than expected. The skull on the table between us had arrived without documentation, without a case file, without anything except the question that follows unidentified skeletal remains everywhere it goes: how old was this person when they died? I had examined the ectocranial sutures for approximately 12 minutes, which is longer than most people spend on them and shorter than people who have never done it tend to imagine, and I gave her a range. Thirty-five to fifty-five years. Not a decade, not a single age, not the kind of number that sounds good in a press conference or resolves cleanly in a database search. A 20-year interval, communicated with what I hoped was calm authority and what she clearly received as a polite form of professional evasiveness.
I have been in this situation more times than I can accurately count, which is itself a statement about the nature of aging research in a discipline that deals professionally with the absence of documentation. The sutures were partially obliterated. The lateral-anterior composite score placed the individual somewhere between “confidently not a young adult” and “probably not yet in the territory where sutures tell us nothing useful at all.” That is the scientific reality of the method. It works, within a range. It also has limits that are, in the published literature, both extensive and specific, and presenting both of those facts with equal honesty is, in my experience, one of the more reliable ways to make a medical examiner feel that she has hired the wrong consultant, even when the consultant is being rigorously correct.
This article is about cranial sutures as an age indicator, which means it is about one of the most methodologically contested and practically indispensable tools in skeletal analysis, about the century of researchers who argued over its reliability without fully resolving the argument, and about why honest uncertainty stated clearly and without apology is more useful to an investigation than false precision that collapses the moment an opposing expert appears in court. It is also, by necessity, about what bones can and cannot tell us, which is a topic that the entertainment industry has never found as entertaining as it deserves.
The Architecture of the Cranial Vault, for People Who Have Not Held One
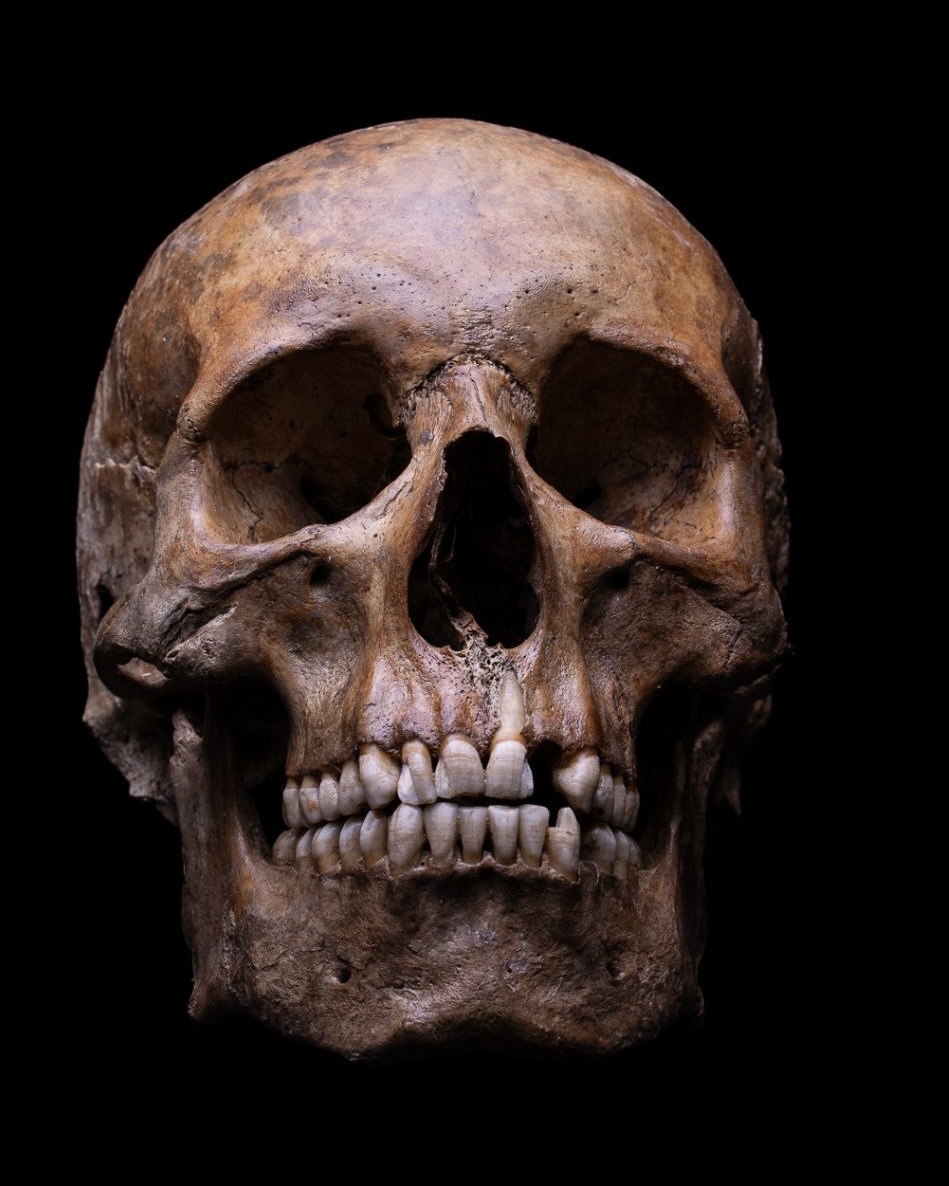
real human skull legal is not a helmet. It is an assembly of 22 bones joined by fibrous connective tissue joints called sutures, with the 3 ossicles of the middle ear bringing the cranially associated total to 29 if one is inclined toward precision, which in this field one generally is. In a newborn, this assembly is deliberately incomplete. The gaps between the bones, the fontanelles, allow the cranial plates to overlap during the compressive adventure of birth and to expand freely during the first years of life, when the brain growing inside them has not yet received any structural limits. The anterior fontanelle, the largest, closes between 12 and 18 months. The posterior fontanelle closes earlier, within the first months after birth.
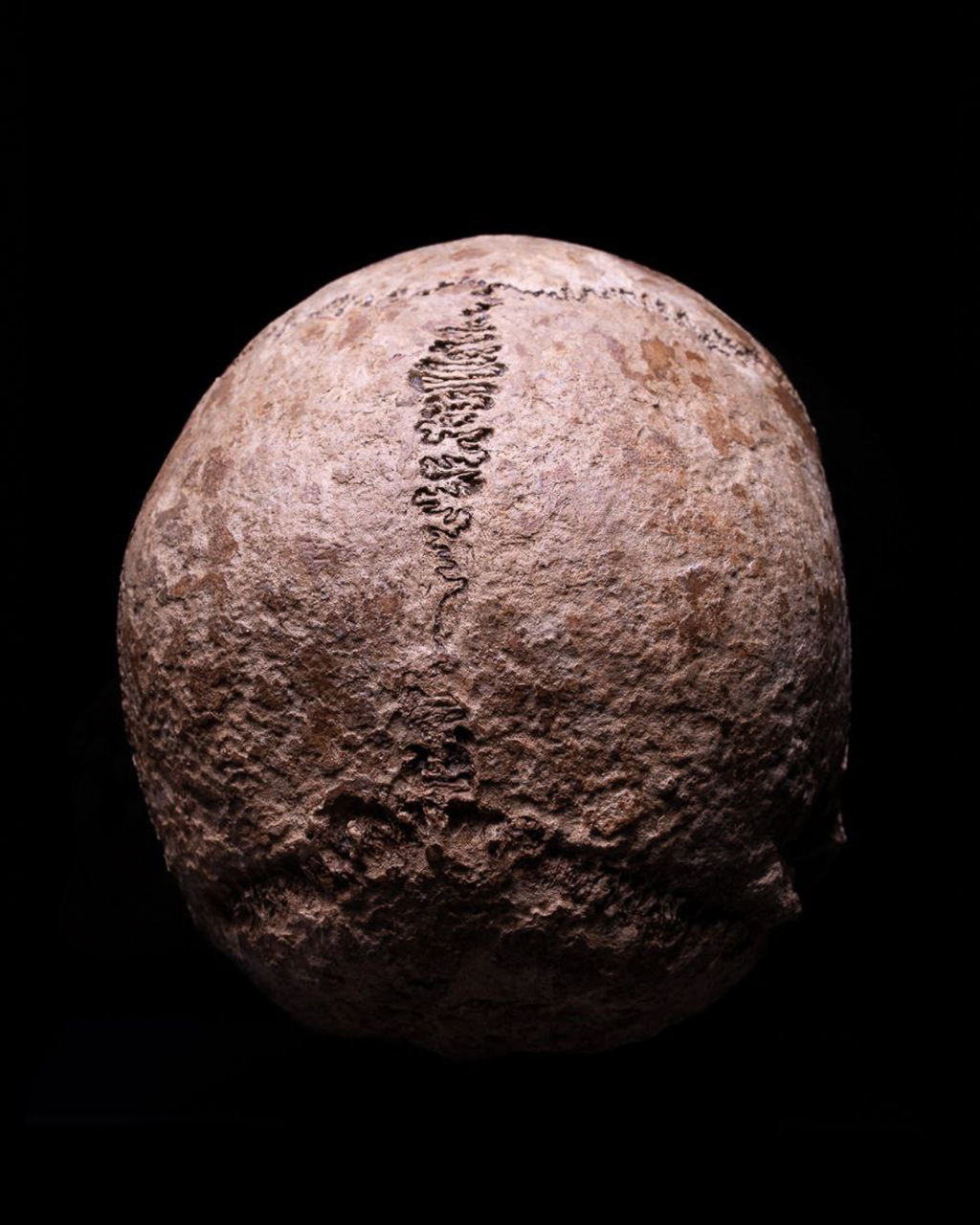
After that, the 22 bones settle into the configuration they will maintain for the rest of a person's life, connected at their margins by sutures that are, in young adulthood, still clearly visible as distinct lines running across the skull's surface like the seams of a sphere assembled by someone working quickly and without reference to the instruction sheet. What makes these seams forensically interesting is what happens to them across the following decades. The fibrous tissue filling the suture gradually becomes mineralized, replaced by bone in a process called obliteration, proceeding at a rate that is broadly predictable in the population sense and maddeningly variable in the individual sense.
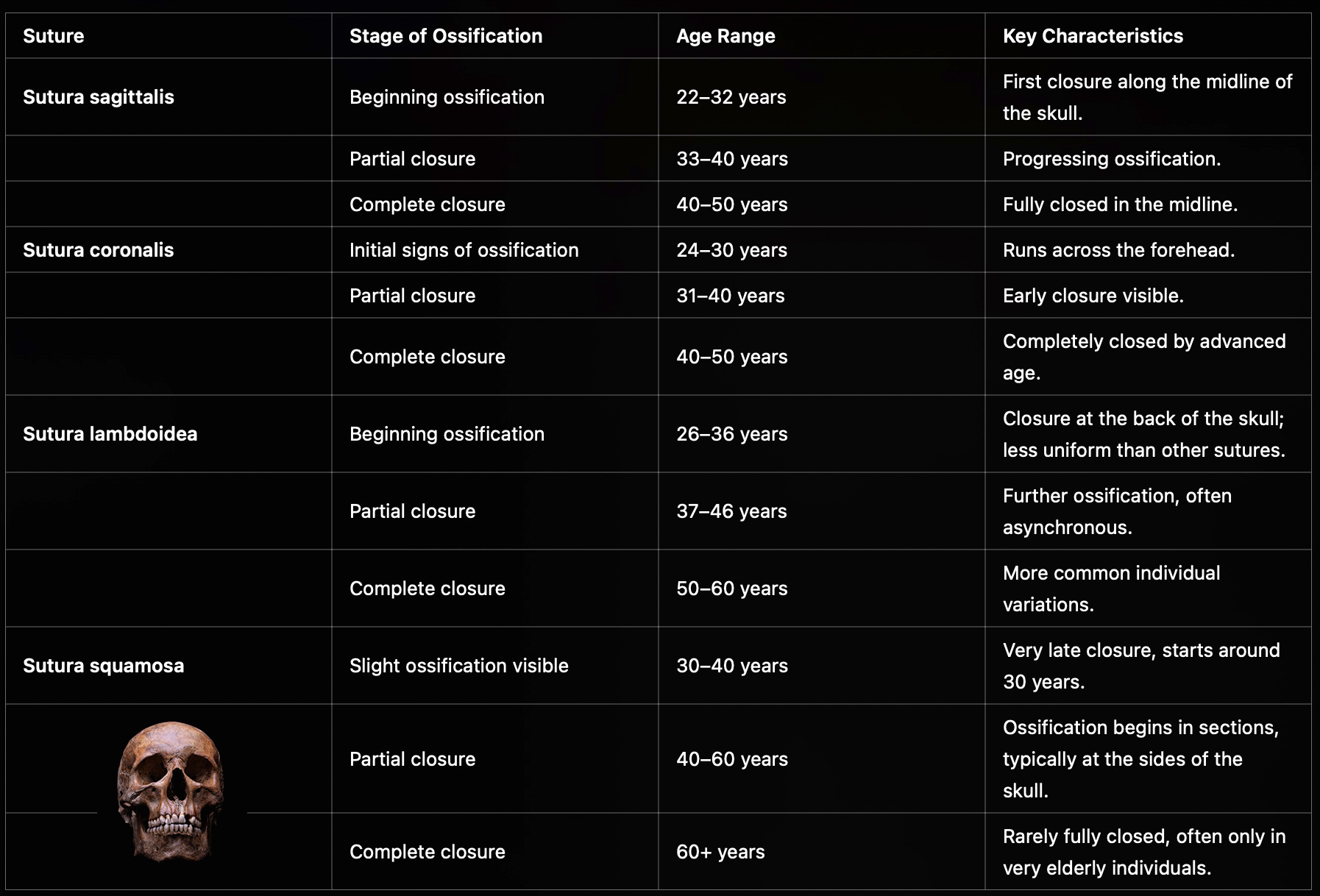
The coronal suture, running transversely across the calvarium where the frontal bone meets the 2 parietal bones, tends to begin showing obliteration earliest, typically in the third and fourth decades of life. The sagittal suture, running along the midline of the skull's roof between the 2 parietal bones, follows a similar timeline. The lambdoid suture at the posterior, where the parietals meet the occipital bone, often closes later and more irregularly. The squamosal suture on the lateral surface of the skull, connecting the temporal bone to the parietal, is generally the last to close and displays the most individual variation of the 4 major systems, which is the kind of sentence that sounds like a minor methodological footnote and is in practice a persistent source of interpretive difficulty.
The biology driving suture obliteration is not fully understood, which is the sort of statement that produces uncomfortable silences at forensic anthropology conferences but which is simply true. Genetics plays a role. Nutritional history plays a role. Hormonal environment across the life course plays a role. Pathological conditions, including chronic infection and certain metabolic disorders, can accelerate or, less commonly, retard the process. Mechanical stress has been proposed as a contributing factor. What all of these influences share is that they act differently in different individuals, producing a range of closure states at any given age that overlaps substantially between adjacent age decades and is wide enough, at the extremes, to accommodate outliers that would embarrass any practitioner who had reported a tight estimate based on sutures alone.


One Hundred Years of Arguing About the Same Lines
The history of cranial suture closure as a forensic tool begins in the 1920s with T. Wingate Todd and D.W. Lyon, who published a series of papers in the American Journal of Physical Anthropology examining suture closure across the Hamann-Todd Osteological Collection in Cleveland, Ohio, a documented skeletal collection assembled primarily from individuals who died without family in the early decades of the 20th century (Todd, T.W., & Lyon, D.W., 1924, Endocranial Suture Closure: Its Progress and Age Relationship, American Journal of Physical Anthropology, 7(3), 325-384). Todd and Lyon's work established the foundational framework: sutures obliterate in a sequence, the sequence correlates with age, the correlation is imperfect, and the uncertainty increases substantially with advancing age. These are findings that subsequent research confirmed, contested, refined, and re-confirmed over the following century, which is either a sign of scientific health or a sign that the foundational uncertainty was more fundamental than anyone initially wanted to acknowledge.
Acsádi and Nemeskéri published their revision in 1970, working from a Hungarian skeletal collection and focusing primarily on endocranial suture closure assessed from inside the skull. Their composite scoring system across 4 vault suture locations argued for improved reliability through aggregation, the logic being that averaging out the variability across multiple measurement sites would reduce the noise inherent in any single one. The logic is sound in principle, and the improvement in practice was real, if more modest than the method's advocates have sometimes suggested.
The revision that current forensic anthropologists actually use came from Richard Meindl and C. Owen Lovejoy in 1985, in 2 companion papers in the American Journal of Physical Anthropology that remain the methodological reference point for contemporary practice (Meindl, R.S., & Lovejoy, C.O., 1985, Ectocranial Suture Closure: A Revised Method for the Determination of Skeletal Age at Death Based on the Lateral-Anterior Sutures, American Journal of Physical Anthropology, 68(1), 57-66). Rather than assessing sutures in their entirety, Meindl and Lovejoy identified 10 specific sites across the vault and lateral-anterior systems where closure could be scored on a simple 0-to-3 scale representing open, minimal, significant, and complete obliteration. Composite scores from 2 groups of sites, the lateral-anterior system encompassing 6 sites at the coronal and pterion region, and the vault system encompassing 4 sites at the sagittal and lambdoid, could then be matched against reference ranges from the Hamann-Todd Collection to produce an estimated age interval.
Meindl and Lovejoy found that the lateral-anterior system outperformed the vault system, that ectocranial scoring outperformed endocranial scoring, and that their age estimates showed no significant relationship with sex or with the Black-White distinction present in the Hamann-Todd documentation. This last finding has been cited frequently as evidence for cross-population applicability of the method, with a generosity of interpretation that the subsequent literature does not entirely justify.
The Hamann-Todd Collection consists primarily of individuals who died in Cleveland, Ohio, between approximately 1912 and 1938. The population diversity in that collection reflects the demographics of an early 20th-century American Midwestern city, which is a specific and limited slice of human biological variation. It does not represent East Asian populations, Southeast Asian populations, South Asian populations, indigenous American populations, or the full range of genetic backgrounds present in the contemporary global forensic caseload. One publishes with the data one has. One should also say clearly, every time, what data one did not have, because the courts one testifies in will eventually contain defendants, victims, and identified remains from all of those populations.
The Critics Were Mostly Right, and That Is Useful Information
There is a tendency in forensic anthropology, as in most applied sciences whose practitioners also serve as expert witnesses, to emphasize the reliability of one's methods rather than their limitations. This tendency is understandable, professionally motivated, and epistemically wrong. A comprehensive 2019 review of cranial suture closure as an age indicator in Forensic Science International, authored by Case and Heilman and published in 2020, examined the accumulated evidence from a century of research and concluded, with a directness that I found professionally refreshing and that some colleagues found professionally confronting, that “the critics who have argued for the unreliability of cranial sutures as estimators of age have mostly won,” while allowing that the indicator retains value when properly contextualized (Case, D.T., & Heilman, J., 2020, Cranial Suture Closure as an Age Indicator: A Review, Forensic Science International, 307, 110105).
Those critics are not a fringe minority. Singer, writing in 1953, argued that the correlation between suture closure and chronological age was too variable for reliable individual assessment. Brooks, in 1955, reached similar conclusions from independent sample data. Masset, in 1989, identified systematic biases: overestimation of age in younger individuals, underestimation in older ones, a pattern that misdirects the method's errors precisely where they cause the most investigative damage. Hershkovitz and colleagues, in 1997, found the relationship between suture closure and chronological age sufficiently irregular to question the method's forensic utility in categorical terms. A validation study on Thai skeletal material found inaccuracy ranges of 13 to 22 years when applying the Meindl-Lovejoy method to a non-Western-European sample, a number worth sitting with for a moment. The method already produces confidence intervals spanning 20 years in many age categories. An additional population-specific error of up to 22 years on top of that produces a result that is technically a range and practically a polite way of saying “somewhere between the early years of working life and the early years of retirement.”
None of this makes the method worthless. It makes it a supporting indicator, not a primary one. In a skull with no other available skeletal evidence, suture closure provides an age interval that narrows the investigative search space compared to having no biological information at all. That is a genuine contribution, even if a more modest one than textbook descriptions tend to suggest. In a more complete skeleton where pubic symphysis morphology, auricular surface changes, dental wear, and cortical bone histology can also be assessed, suture closure adds one data point to a multifactorial assessment whose composite precision exceeds any single indicator's individual performance. That is how it should be used. That is the context in which its value is real and its limitations are manageable.
The Pelvis Is Better. The Skull Is More Often Present.
The pubic symphysis and the auricular surface of the ilium are the most reliable age indicators available in the adult skeleton. Both undergo morphological changes across adulthood that correlate with chronological age more consistently than suture closure does, with lower error rates and less population-specific variability in their performance. The Suchey-Brooks method for pubic symphysis morphology and the Buckberry-Chamberlain method for auricular surface assessment are the current methodological standards for those regions, and both outperform suture closure as single-indicator age estimation tools by a margin that the forensic anthropology literature does not debate.
The problem is survival. The pubic symphysis sits at the front of the pelvis in a region anatomically exposed to the taphonomic processes that destroy skeletal remains: animal scavenging, soil chemistry, flooding, mechanical disturbance from roots, agricultural equipment, and construction work. The cranium, by contrast, is architecturally dense, mechanically robust, and protected by its rounded geometry from many of the forces that fragment the appendicular skeleton and scatter the pelvis across a scene. In the practical experience of anyone who has worked at outdoor discovery sites, the skull is more often recovered, more often intact, and more often the primary available evidence than the pelvis. This is not a statement about relative scientific value. It is a fact about which bones survive long enough to be examined.
William Maples, who directed the C.A. Pound Human Identification Laboratory at the Florida Museum of Natural History in Gainesville until his death from a brain tumor in February 1997, and whose casework included the identification of Francisco Pizarro's remains and participation in the Romanov skeletal investigation, understood the strategic function of suture analysis in precisely this context (Maples, W.R., & Browning, M., 1994, Dead Men Do Tell Tales, Doubleday). Sutures do not solve a case. They define the investigative window. A 20-year interval covering ages 35 to 55, applied to a missing persons database in a specific region over a specific historical period, produces a manageable set of candidates. The final identification, in competent practice, always comes from something more definitive: dental records, DNA, fingerprints, or a combination. The sutures open the door; they do not close the case, and a practitioner who presents them as if they do is preparing a cross-examination that will not conclude pleasantly for anyone involved.
In my own practice, a construction site in northern Germany produced a cranium at 2 meters depth, without accompanying skeletal material. The vault sutures showed partial obliteration. The lateral-anterior composite score fell in the range consistent with 35 to 55 years. The ectocranial surface showed none of the periostitic changes that would suggest infectious disease had accelerated closure atypically. Secondary dentine deposition in the visible roots contributed a second data point that tightened the estimate somewhat toward the 40-to-50-year band. I reported a range, with the methodology documented and the limitations stated. The Landeskriminalamt cross-referenced it against regional missing persons records and identified a 44-year-old man who had disappeared from that municipality 11 years earlier under circumstances that had never been clarified. The final identification came from DNA comparison with a first-degree relative. The sutures did not identify anyone. They narrowed the search to a scale that could be searched.
The Reference Sample Problem That Did Not Go Away With Successive Revisions
The Hamann-Todd Collection is one of the foundational documented skeletal collections in North American physical anthropology, and it is a collection of people who died in Cleveland, Ohio, in the early decades of the 20th century under specific historical conditions. The individuals in it arrived there through the demographic processes that produced the composition of an early American industrial city: migration from specific regions of Europe, internal migration from specific regions of the United States, and the economic conditions that determined who died without family at a public institution and whose remains were therefore available for anatomical study. The genetic diversity of this collection is real and limited simultaneously.
The Thai validation study is the most cited illustration of what happens when one applies a method developed on this collection to populations distant from it: 13-to-22-year inaccuracy ranges, with systematic bias in both directions. Comparable population-specific performance degradation has been documented in Japanese, Indian, and Turkish skeletal samples. The pattern is consistent. The method was developed on a collection that does not represent the full range of human biological variation, and its performance on populations distant from that reference diminishes in ways that are predictable in direction, if not always in magnitude.
The honest response is not to abandon the method in non-European forensic contexts. It is to document the mismatch explicitly, apply wider confidence intervals that reflect the additional population-specific uncertainty, and present the findings as one among several parallel lines of evidence rather than as a primary determination. This response requires a level of methodological self-disclosure that not every practitioner applies consistently. That inconsistency has consequences, because the courts where these findings are presented do not always have the forensic science literacy to demand the disclosure that the practitioner should be providing voluntarily. The discipline's credibility depends on practitioners providing it anyway.
What CT Scanning Changes, and the One Thing It Does Not
Post-mortem computed tomography has introduced a genuinely useful new dimension to suture analysis. The internal architecture of a suture, the distribution of ossification along its length, the differential pattern of ectocranial versus endocranial closure, and the 3-dimensional interdigitation between opposing bone edges are all visible in CT data at a resolution that exceeds what direct examination of a dry skull surface provides. Several research groups have applied CT-based scoring to cranial suture closure and found results broadly consistent with the traditional ectocranial method, while gaining additional information about the 3-dimensional structure of the obliteration process that the original surface-scoring approach could not access.
This is a genuine advance in documentation and characterization. It also offers a significant operational advantage in cases where the skull must be preserved as evidence or returned to a family: the sutures can be documented non-destructively, in full 3-dimensional detail, before the skull leaves the forensic environment. Post-mortem CT is now routinely used in forensic anthropology units that have access to radiology equipment, and this documentation capacity is a real improvement over the traditional method's requirement for direct handling.
What CT does not change is the one thing that matters most to the accuracy question. The variability in cranial suture closure rates between individuals is a biological property of the sutures themselves, not a measurement artifact produced by the limitations of visual scoring. A skull that shows ambiguous partial obliteration at age 40 and one that shows the same pattern at age 55 look ambiguously partially obliterated in CT just as they do to the naked eye. Better imaging of a biological variable does not reduce the range of that variable in the population. The confidence intervals that result from CT-based scoring are not dramatically narrower than those produced by the traditional ectocranial method. The fundamental uncertainty remains, more clearly described, more precisely documented, and equally fundamental.
A Warning for Those Who Prefer Their Bones More Decisive
There is a television programme format, familiar to anyone who has not successfully avoided it, in which a forensic specialist examines a skull for approximately 45 seconds and announces the victim's age to within 2 years, the sex with certainty, and the probable cause of death before the next scene. I have maintained for some years a complicated relationship with this format. The bones that arrive in actual forensic examination rooms are usually older, more fragmented, and considerably less cooperative than the ones handled by actors who have rehearsed looking grave while holding prop crania. The examinations take longer. The conclusions are narrower. The reports are more qualified than the ones delivered to fictional investigators who need the answer before the next commercial break.
The gap between what forensic anthropology can deliver and what courts, investigators, and occasionally television producers expect it to deliver is not always bridged by better science. Sometimes it is bridged by practitioners who have learned to present wide intervals with sufficient confident body language that nobody in the room asks the follow-up questions that would reveal how wide the interval actually is. This is a human solution to a communication problem, and it has produced some well-documented complications in courts that eventually did ask the follow-up questions.
Suture closure is particularly susceptible to this gap because it is visually the most accessible age indicator and the one most intuitively graspable by non-specialists. A clearly open suture reads as young. A clearly obliterated suture reads as old. The forensic anthropologist standing in the middle, who sees partial closure at a site where the reference data show substantial overlap between 3 adjacent age decades, owes the investigation an honest account of what that overlap means for the precision of any estimate derived from it. That account is rarely the one that satisfies an investigator who has driven 2 hours to hear something more specific, and it is always the one that holds up when the case goes to trial and the defense has retained its own expert who has read the same literature.
The alternative, stating more certainty than the method supports, is not a service to the investigation or to the family waiting for an identification. It is a debt that accumulates interest until cross-examination, at which point it is collected in full, in public, with both experts' methodological disclosures on the record and the jury watching.
The Interval Is the Answer
The skull on the examination table does not know its own age, and it cannot be made to disclose a more precise answer by being examined more forcefully or described with more confidence. What the biology recorded in the bone is the trajectory of an obliteration process that ran at the rate the individual's specific combination of genetics, nutritional history, hormonal environment, and imperfectly understood additional factors produced. The interval I report is not the age this person died. It is the age range within which the biological evidence is consistent with their having died, given the reference sample, the scoring system, the population match, and the individual variability that the method cannot eliminate.
That interval is honest. Its honesty is the minimum obligation that the discipline owes both the investigation it serves and the person whose remains are on the table, who cannot correct a misidentification, and whose family, if they are still searching, deserves the most accurate answer the evidence supports rather than the most confident one the practitioner can construct.
In the next piece on this site, I will turn to the pubic symphysis and the auricular surface, the age indicators that outperform suture closure in reliability and underperform it in survival, and therefore form with it a complementary pair that defines what skeletal age estimation actually is in practice: not a single authoritative reading, but a conversation between multiple imperfect indicators that together tell a more complete story than any of them tells alone. Those who have read this far have already demonstrated the patience for that conversation. The ones who needed a single number left at the end of the previous paragraph, and I wish them well with the television format, which will continue to provide it without any of the qualifying clauses that make the actual science both more honest and more useful.
References
- Case, D.T., & Heilman, J. (2020). Cranial suture closure as an age indicator: A review. Forensic Science International, 307, 110105. https://doi.org/10.1016/j.forsciint.2019.110105
- Maples, W.R., & Browning, M. (1994). Dead men do tell tales: The strange and fascinating cases of a forensic anthropologist. Doubleday.
- Meindl, R.S., & Lovejoy, C.O. (1985). Ectocranial suture closure: A revised method for the determination of skeletal age at death based on the lateral-anterior sutures. American Journal of Physical Anthropology, 68(1), 57-66. https://doi.org/10.1002/ajpa.1330680106
- Meindl, R.S., Lovejoy, C.O., Mensforth, R.P., & Barton, T.J. (1985). Multifactorial determination of skeletal age at death: A method with blind tests of its accuracy. American Journal of Physical Anthropology, 68(1), 1-14. https://doi.org/10.1002/ajpa.1330680102
- Todd, T.W., & Lyon, D.W. (1924). Endocranial suture closure: Its progress and age relationship. Part I: Adult males of white stock. American Journal of Physical Anthropology, 7(3), 325-384. https://doi.org/10.1002/ajpa.1330070314
Is It Legal to Own a Real Human Skull? Yes, Subject to 3 Conditions
Private possession of a real human skull is not prohibited in Germany. Three conditions decide the question, and…

The Science and Ethics of Age-Gap Attraction: Why Older Men Are Drawn to Younger Women, and Where the Line to Crime Runs
A forensic examiner lays out the evolutionary psychology and the data from 130 countries: the algorithm of age-gap…

The Pressure Fallacy: What Pink Teeth in the Dead Really Reveal, and What They Do Not
A forensic investigation through 200 years of literature, prompted by three cases, two of which I examined myself,…